tree in bud opacities seen in
182122 The early changes of lower lobepredominant peribronchial thickening and peribronchial GGOs or tree-in-bud opacities are more readily appreciated on a lateral plain film or with greater sensitivity by chest CT although. Bronchial stenosis is seen in 1040 of patients with active tuberculosis 27 and is best demonstrated with CT which usually shows long segment narrowing with irregular wall thickening luminal obstruction and extrinsic compression 30.
2
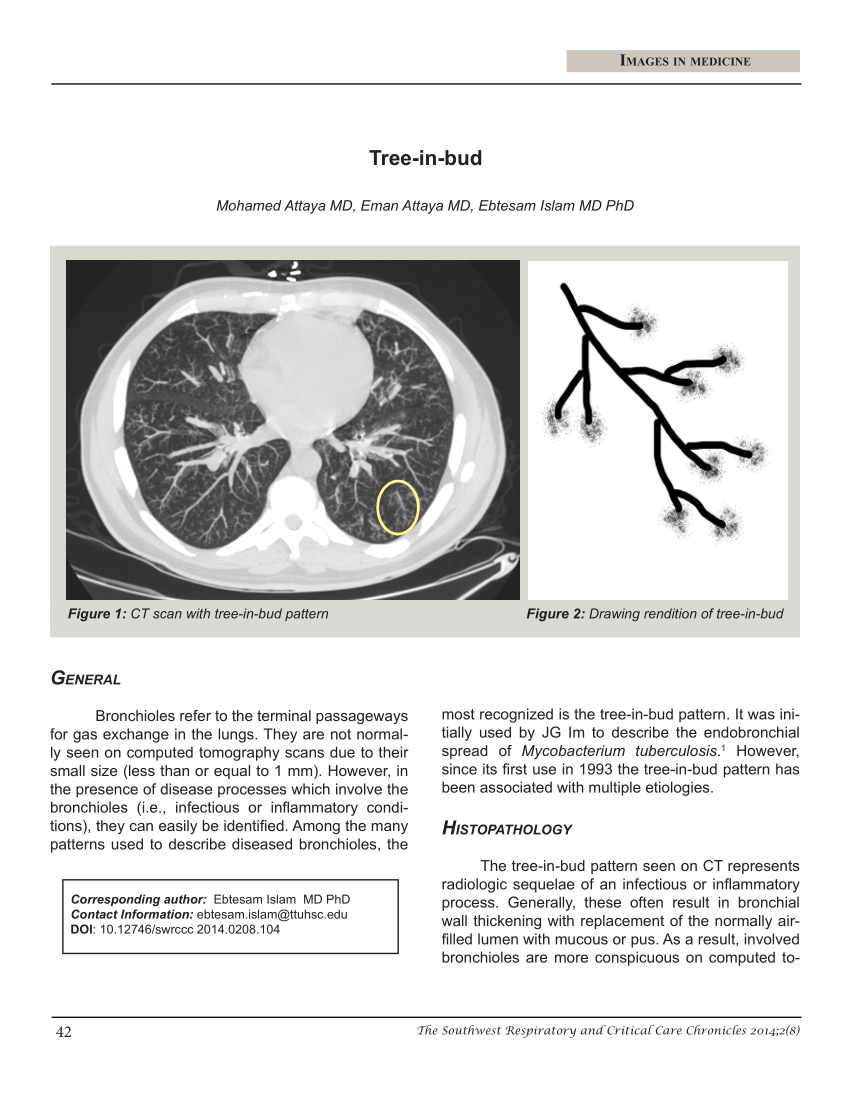
Multiple causes for tree-in-bud TIB opacities have been reported.
. The most common HRCT patterns include the septal reticular ground-glass opacity crazy paving pattern mixed ground-glass opacity and reticular nodular tree-in-bud pattern nodular without tree-in-bud pattern nodular with ill-defined centrilobular reticulonodular cystic mixed cystic with ground-glass opacity decreased attenuation and. Typically the centrilobular nodules are 2-4 mm in diameter and peripheral within 5 mm of the pleural surface. TIB opacities were seen in association with bronchiectasis in 30 123 of 406 of cases and with an apical-predominant disease in 25 10 of 406 cases.
Chronic Kerley B lines may be caused by fibrosis or hemosiderin deposition caused by recurrent pulmonary edema. It is a non-specific sign with a wide etiology including infection chronic interstitial disease and acute alveolar disease. It is usually visible on standard CT however it is best seen on HRCT chest.
Patients recovering from COVID-19 can have persistent symptoms and CT abnormalities of variable severity. At 3 months after acute infection a subset of patients will have CT abnormalities that include ground-glass opacity GGO and subpleural bands with. The acute course of COVID-19 is variable and ranges from asymptomatic infection to fulminant respiratory failure.
They are suggestive for the diagnosis of congestive heart failure but are also seen in various non-cardiac conditions such as pulmonary fibrosis interstitial deposition of heavy metal particles or carcinomatosis of the lung. Tree-in-bud sign is not generally visible on plain radiographs 2. Because of the wide variability in the disease process presenting complaints will vary.
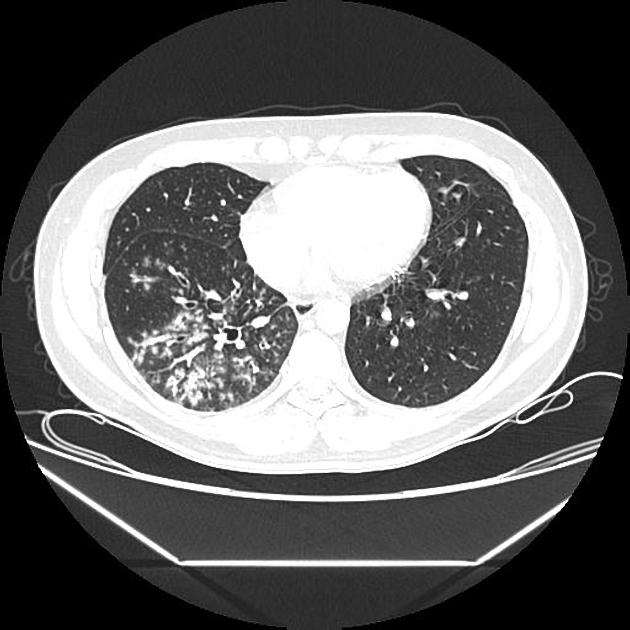
However to our knowledge the relative frequencies of the causes have not been evaluated. In the right mid-lung nodular opacities are in a tree-in-bud distribution suggestive of endobronchial. Adnexal or orbital disease may be seen with preauricular lymphadenopathy.
Of this group airspace disease is the most common finding seen in 90 of patients with CT-documented pneumonia. Small patchy peripheral opacities are also present in the left lower lobe. It also results in tree-in-bud opacities and traction bronchiectasis particularly of the upper lobes.
COVID-19 Corona Virus Disease-19 is a zoonotic illness first reported in China in December of 2019 linked to a seafood wholesale market in the city of Wuhan the capital city of Hubei province1 2 On March 11 2020 COVID-19 was declared a global pandemic by World Health Organization WHO3 having rapidly spread by human to human. In the remaining 67 273 of. Ground-glass opacificationopacity GGO is a descriptive term referring to an area of increased attenuation in the lung on computed tomography CT with preserved bronchial and vascular markings.

Scielo Brasil Tree In Bud Pattern Tree In Bud Pattern

Ct Scan Of Chest Revealing Scattered Tree In Bud Opacities In Both Download Scientific Diagram
Pdf Tree In Bud

Tree In Bud Pattern Radiology Case Radiopaedia Org

Tree In Bud Sign Lung Radiology Reference Article Radiopaedia Org
2

Hrct Scan Of The Chest Showing Diffuse Micronodules And Tree In Bud Download Scientific Diagram

Tree In Bud Sign Lung Radiology Reference Article Radiopaedia Org

Tree In Bud Pattern Radiology Case Radiopaedia Org
2

Pdf Tree In Bud Semantic Scholar
View Of Tree In Bud The Southwest Respiratory And Critical Care Chronicles
2

Tree In Bud Pattern Pulmonary Tb Eurorad
2
Tree In Bud Appearance Radiology Case Radiopaedia Org
2

Computed Tomography Of The Chest Showed Nodular Opacities With Tree In Download Scientific Diagram

Tree In Bud Pattern Pulmonary Tb Eurorad